|
Oct. 9 (Tue.), 2001
|
| 8. Studies comparing effects of early treatment |
|||||||
|
The orthodontic literature will be reviewed to compare effects of early treatment.
A. Comparison of treatment effects between the primary and mixed dentitions A removable mandibular retractor was used in the study to compare its effect between the primary and mixed dentitions. It was concluded that a greater improvement of jaw relationship was obtained with early treatment in the primary dentition. B. Comparison between the early and late mixed dentitions A comparison was made between 7-year-olds and 11-year-olds with a chin cup.
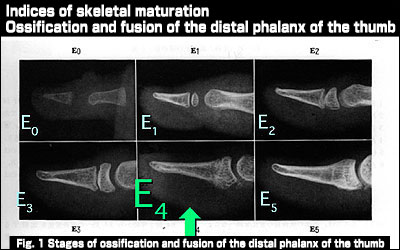
One study supports the effectiveness of early treatment, while the other questions the validity of early treatment. How should we clinicians approach to early treatment from the standpoint of creating oral health with a good occlusion? The first controversy involves the view that even a skeletal Class III malocclusion can be corrected with active early treatment and the opposing view that a true skeletal Class III problem, if treated early, would relapse with growth and be difficult to treat by orthodontics alone. There is another controversy. Some people argue that a dento-alveolar or functional Class III malocclusion would progress to skeletal mandibular prognathism if left untreated. Others attribute this to the failure to accurately diagnose skeletal mandibular prognathism at the time of the initial examination, saying that genetic predisposition cannot be altered with orthodontic treatment. How should we deal with these controversies? I would like to discuss them in more detail. Identification of the stage of growth and development Body height increase and skeletal maturity can be used as indices of growth and development. Especially, the fusion of the distal phalanx of the thumb can be easily identified on a standard dental radiograph. Stage E-4 where fusion is 3/4 complete with the epiphysis wider than the diaphysis is the period of growth deceleration past the pubertal growth peak, serving as an important index for determining when to start treatment, especially of Angle Class III malocclusions. |
|||||||
  |
|||||||
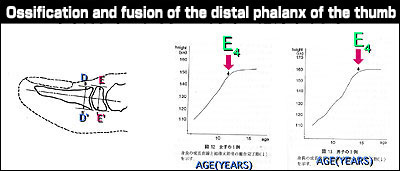
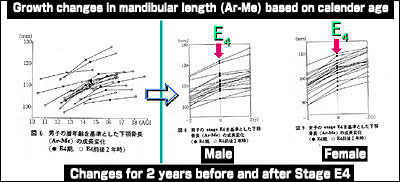
| Among the available indices of skeletal maturity, the ossification and fusion of the distal phalanx of the thumb is a useful biologic indicator. Stage E4 is the terminal stage of the fusion, which is more than 3/4 complete with the epiphysis being wider than the diaphysis as shown in the figure. (Shigeki Gotoh: Changes with age in ossification and fusion of the distal phalanx of the thumb, Journal of Japan Orthodontic Society 46: 534-546, 1987). The figure shows a growth curve of the mandible (Ar-Me) for 2 years before and after Stage E4 based on the calendar age. |
|||||||
 |
|||||||
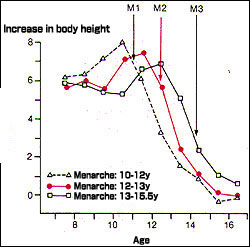
| (Takamasa Kondo: Growth pattern of the cranio-maxillo-facial complex at the terminal stage of fusion of the distal phalanx of the thumb, Journal of Japan Orthodontic Society 50: 293-302, 1991) Annual increase in body height and menarche are also useful biologic indicators. |
|||||||
 |
|
|
|