|
Oct. 9 (Tue.), 2001
|
 |
|
|
9. Differential diagnosis of Class III malocclusions 4
|
ü@Results of the study -2 Summary of cephalometric changes with time
5. Linear and angular measurements were made on the cephalograms taken at the three time points (initial examination, appliance removal and occlusal stability) in Group N with a normal overjet at occlusal stability and Group R with an anterior crossbite at occlusal stability.
As a result, the stability of crossbite correction tended to be higher as the SNA, SNB, ANB, AO-BO, A-B plane, ODI and APDI values approached to the norms. Particularly, L1 inclination, AO-BO, ODI and gonial angle were considered to be useful indicators for differential diagnosis.
|
ü@(Results of t-test for comparison between Group N and Group R: p<0.005)
|
|
|
ODI, which showed a significant difference in a preliminary study, is an indicator of cranio-maxillo-facial vertical dimension. ODI was analyzed in relation to APDI. Some of the patients in Group R had a small ODI although APDI was not so large.
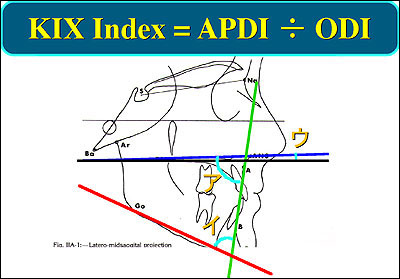
Based on this data, a new index called KIX Index, which is derived by dividing APDI by ODI, was applied to the study subjects to determine its usefulness as an index for differential diagnosis.
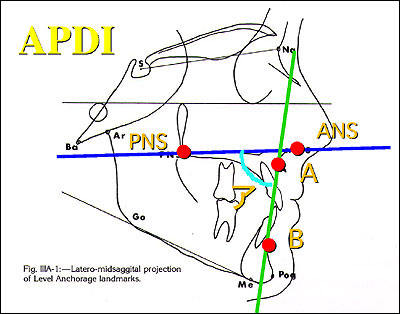
APDI: Anteroposterior Dysplasia Indicator
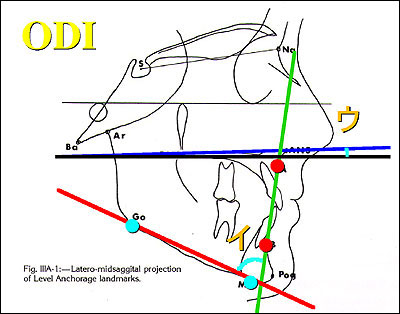
ODI: Overbiteis Depth Indicator (by Dr. Kim).
APDI stands for Anteroposterior Dysplasia Indicator proposed by Dr. Young H. Kim.
|
|
ODI stands for Overbiteis Depth Indicator.
|
|
APDI was divided by ODI to derive a new index called KIX Index.
|
|
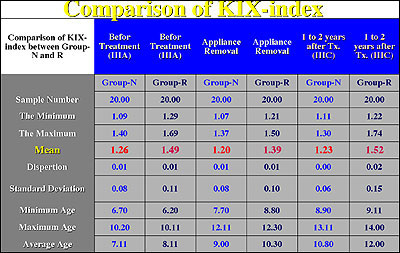
KIX Index was calculated in Group N and Group R.
|
|
As a result of t test, significant differences in KIX Index were noted between the two groups at all the three time points, suggesting that KIX Index may be a useful index for differential diagnosis of skeletal Class III malocclusions at initial examination.
Changes in KIX Index with time were investigated in three cases subjected to orthognathic surgery due to excessive growth of the mandible during the observation period. All the three cases had a KIX Index of around 1.5, indicating a difficulty of crossbite correction with early treatment and a high probability of requiring Phase II treatment or orthognathic surgery. In fact, KIX Index worsened with time in these patients with marked forward growth of the mandible and increased negative overjet. Furthermore, there was a limited backward and downward growth of Ar point, a landmark for the temporomandibular joint area, which failed to compensate for the excessive forward growth of the mandible within the growing maxillo-facial complex.
KIX Index can be used as an indicator of orthognathic surgery. There seems to be a greater need for orthognathic surgery when the index exceeds 1.5. An increase in KIX Index past 1.5 means an increased APDI and a decreased ODI, which in turn indicates an increase in Class III or open-bite tendency. KIX Index of 1.5 is derived from APDI of 90 and ODI of 60, for example. These values indicate a severe Class III malocclusion with a severe open bite.
Caucasian mean: 1.09
Japanese mean: 1.13
|
Patients who do not respond to crossbite correction in the early mixed dentition and who show an increase in KIX Index to above 1.5 and up to 2.0 are very likely to be indicated for orthognathic surgery. Under these circumstances, the doctor needs to make extra efforts to form a rapport with the patient and family and give special consideration to informed consent and second opinion.
|
|
|